Every system has surges in volume, whether they are predictable or unpredictable surges. Most facilities were not designed to handle either type of surge – it’s simply not cost effective. But staff can make the best of their inflexible facilities by knowing what to do in case of a surge in volume.
There is a difference between reacting to a surge already underway and anticipating a surge in advance.
For some of us the “what if” scenario rarely happens, or may happen with some degree of predictability, like annual flu season. In these cases, staff often assume that it’s “business as usual” and we hope for the best!
So what is the best way to manage patient volume surges?
It is possible to predict patient volume surges right down to the impact on a per shift basis with a fair amount of certainty. Analyze daily census data to identify the busiest days of the week and hours of the day. Once you delineate a trend, you can begin to prepare for it.
Ways to Prepare for Anticipated Volume Surges
- Adopt a peak census staffing model by day and by hour. Allocate ED physicians and mid-level providers, transporters, and support staff such as volunteers and patient representatives.
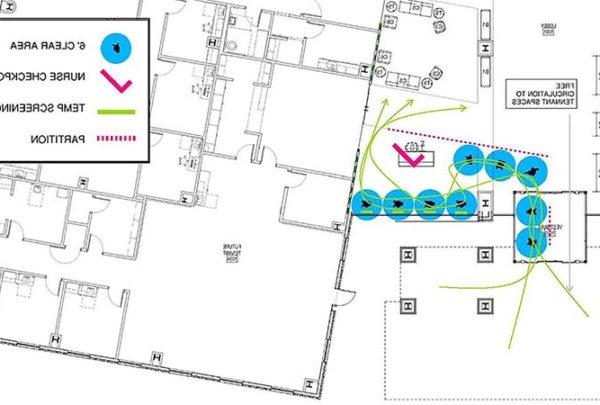
- Streamline the intake process to limit any patient bottlenecks at a point of entry. Strive to expedite the arriving patient to the right place in the right amount of time for the right type of care. This way, surges, when they occur, are less impactful.
- Prepare the department by ensuring supplies are at hand, and carts from Central Supply are fully stocked and readily available.
- Alert downstream departments: inpatient units, surgery, ICUs, imaging, lab, RT, EVS, Materials Management, Pharmacy, Security, and Central Supply. As the ED is the “front door” to the hospital, surges originate here.
- Consider external/internal disaster response processes for insights on managing an unexpected surge. During biannual disaster planning and drills, staff can role-play “what-if” scenarios, and use the results as the basis for standard procedures. Inpatient departments must also ingrain surge procedures.
Sometimes, a bolus of patients arrives suddenly that you could not predict through historic arrival patterns. If you didn’t see it coming, how do you manage?
Unexpected or short term surges such as the recent Ebola outbreak or severe weather challenge providers on many fronts. Managing an influx of patients burdens physical space and operational processes. An unexpected surge in patient volume can tax staffing ratios, staff education, and equipment and supplies.
Ways to Increase Capacity in an Unexpected ED Surge
- Focus on the patients you can discharge first. Direct them off campus as soon as possible.
- In the ED, use a results-waiting model in the short term. Here, vertical and some horizontal patients can complete the portion of their care that does not require a bed. This way the bed can become available more quickly for subsequent patients.
- Pull the lowest acuity patients out of the mix. Direct them to a predetermined area within the hospital that is set up to manage care and treatment of lower acuity patients. This location can also manage the “walking wounded” or low acuity patients from the surge in ED patient volume. This effort will help to free up physical capacity in the ED immediately.
- Pull the Charge Nurse into staff mix for the short term. This works if the ED Nursing Director or Manager can assume the role of Charge RN.
- Deploy additional in-house technical support staff (may include transporters) and extra in-house clerical staff.
- Direct house-wide staff to the department most in need. For example, Transporters, Techs, or even nurses may need to work in the ED to care for patients.
As a last resort, stage patients in the hallways. Make sure hallway patients are less acute, and/or have already had treatment initiated. It is best for patients in need of medical management to receive that care on an inpatient unit. Sometimes the “inpatient mindset” assumes that the presence of doctors and nurses makes the ED or PACU an acceptable place to house an admitted patient. We maintain that EDs, PACUs, or other staging areas are not staffed, equipped, or physically structured to deliver the level of inpatient care that admitted patients require.
In Part 2: How to increase capacity in an unexpected inpatient unit surge, plus “big picture” ideas.